
RESCUE ENDOTRACHEAL TUBE (ETT)
Allows intubation through a laryngeal mask airway and subsequent removal of the laryngeal mask airway with continuous airway security, protection and ventilation
The laryngeal mask airway is recognised as one of 3 ‘lifelines’ (face mask, supraglottic airway and endotracheal tube) of the Vortex approach for the can't intubate, can't oxygenate situation (CICO) situation able to fulfil the goal of alveolar oxygen delivery.
Endotracheal intubation through the laryngeal mask airway fulfils the secondary goals of airway protection, airway security and carbon dioxide elimination.
Ideal for use with fibre optic (4), (5) or blind intubation (2) through a laryngeal mask airway.
The rescue ETT is specifically designed for intubation through the laryngeal mask airway over a fibre optic broncoscope.
Suitable to use through mostlaryngeal mask airways as the airway tubing connected to the endotracheal tube gives sufficient length to position the endotracheal tube at a safe distance below the vocal cords.
No stabilizing rod is required.
Reduced hang-up on laryngeal structures due to:
Posterior facing bevel
Curved atraumatic tip abutting against the fibre optic bronchoscope
resulting in increased first pass intubation and reduced laryngeal trauma.
No Interruption in ventilation while withdrawing the laryngeal mask airway over the ETT.
FOB may be left in place, confirming position of ETT is maintained while the laryngeal mask airway is withdrawn.
Risk of accidental extubation while removing the laryngeal mask airway is reduced.
Rescue ETT have high volume low pressure cuffs suitable for long-term intubation and reducing tracheal barotrauma.
Available in both clear PVC and reinforced PVC tubing suitable for ICU or oro-maxillo-facial surgery. Clear PVC ETT is safe for use when a CT or MRI scan is required.
Reinforced PVC ETT is compatible with the Genesis oral/nasal interchangeable ETT
Affordable. Single use. Presented in sterile pack.
Studies that support the use of the Rescue Endotracheal Tube include:
Most standard endotracheal tubes (ETT) are too short to guarantee tracheal intubation: 52
Intubation with the endotracheal tubes bevel facing posteriorly: 59



INDICATIONS
A 'can't-intubate-can't-oxygenate' (CICO) scenario when a laryngeal mask has been placed as a rescue device and works well enough to oxygenate the patient, but there is a need for endotracheal intubation.
After several unsuccessful intubation attempts with direct laryngoscopy
After unsuccessful intubation attempts with video laryngoscopy
Elective use to train for using the technique in an emergent CICO scenario
Conversion from laryngeal mask to endotracheal tube intraoperatively, for example;
where anaesthesia was started with a laryngeal mask but the device subsequently fails/ the seal fails
when muscle relaxation becomes necessary and the anaesthetist does not feel confident to ventilate a paralysed patient with a laryngeal mask
CONTRAINDICATIONS
Patients with an aspiration risk
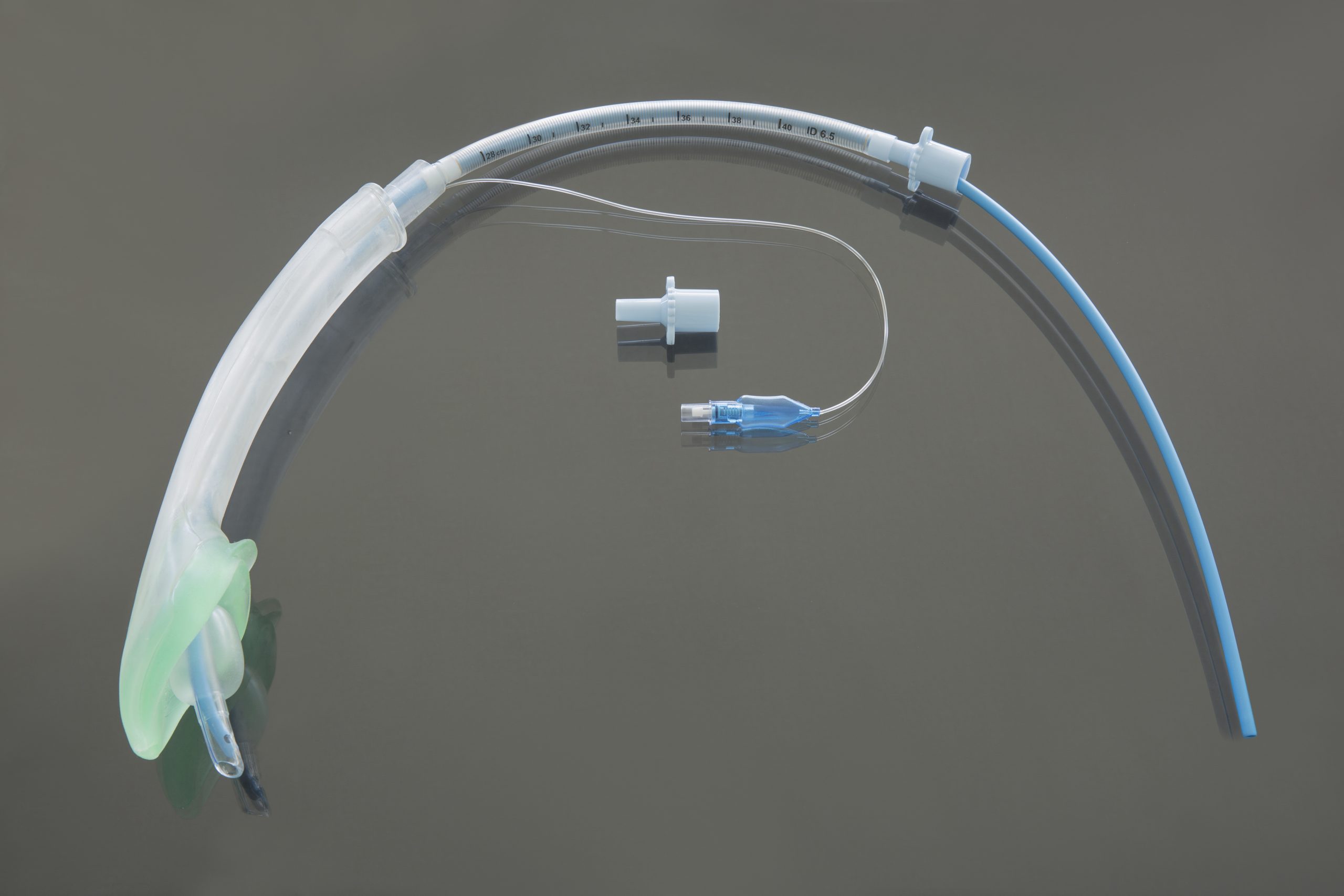
THE RESCUE ETT IS PRESENTED AS A PACK CONTAINING:
Modified endotracheal tube with a posterior facing bevel, curved atraumatic tip and removable 15mm ISO connector
Airway tubing having a fixed 15mm ISO connector at the proximal end and a connector to mate with the distal end of the endotracheal tube
GENESIS RESUCE ETT IS AVAILABLE WITH REINFORCED AND CLEAR PVC ENDOTRACHEAL TUBES.
Modifications made to the endotracheal tubes:
The length of the endotracheal tube connected to the airway tubing is sufficient that the endotracheal tube may be passed through the shaft of the laryngeal mask airway and protrude far enough beyond the laryngeal mask airway to position the ETT cuff safely below the vocal cords.
The bevel is posterior facing with a curved atraumatic tip providing a greater initial success rate of intubation and a preventing hang up on laryngeal structures. The curved atraumatic tip abutting against the fibre optic bronchoscope eliminating the gap causing laryngeal hang-up.
The 15mm ISO connector is removable
The inflation line connecting the cuff of the ETT to the pilot balloon and inflation valve is of sufficient length to allow the laryngeal mask to be removed over the ETT and the ETT disconnected from the Airway tubing before the inflation line, pilot balloon and inflation valve are delivered through the shaft of the laryngeal mask airway.
The PVC has a soft consistency preventing the need for thermosoftening.
A METHOD OF USE WITH A FIBRE OPTIC BRONCHOSCOPE (FOB)
The laryngeal mask airway is used to secure the airway, the anaesthetic machine connected, ventilation and oxygenation are confirmed.
The ETT and the airway tube must be easily disconnected. If the connection is too firm, add water soluble lubricant to the connector.
The appropriately sized rescue ETT is selected (the ETT selected must not be forced through the shaft of the laryngeal mask airway as damage to the cuff if the ETT may occur)
The 15mm ISO connector removed from the ETT and is connected to the Airway tubing. The proximal end of the ETT and cuff is well lubricated.
A FOB with a working length of at least 60cm and sufficient diameter to abut against the curved atraumatic tip of the ETT is chosen.
An self-sealing connector with a sidearm is placed over the 15mm connector of the airway tubing
This complex is then loaded over the FOB with the FOB tip just proximal to the tip of the ETT.
The laryngeal mask airway is disconnected from the anaesthetic machine. The ETT/airway tube is then connected to the anaesthetic machine and the distal ETT inserted into the shaft of the laryngeal mask airway. The cuff of the ETT is inflated in the shaft of the laryngeal mask airway once the ETT tube tip is 2cm out of the distal laryngeal mask airway aperture (e.g. with a #4 I gel laryngeal mask airway shat length =19cm, when ETT is at 21cm measured at the proximal end of the laryngeal mask airway) allowing continued ventilation.
The FOB is then advanced through the vocal cords and into the trachea.
The cuff of the ETT is deflated and the ETT /airway tubing is railroaded over the FOB until the cuff of the ETT is a safe distance below the vocal cords and the cuff is reinflated.
The ETT/airway tubing is stabilized. The laryngeal mask airway cuff is deflated and it is withdrawn carefully over the ETT/airway tube.
It is recognised that physician preference may allow the Rescue ETT to be introduced through an laryngeal mask airway in a variety of ways.
After confirming that the ETT is still correctly positioned the FOB is removed.
The ETT and airway tube are disconnected, the 15mm ISO connector reinserted into the distal ETT and the anaesthetic machine is connected.
The airway tube is removed from the shaft of the laryngeal mask airway and then the inflation line, pilot balloon and inflation valve are delivered through the shaft of the laryngeal mask airway.
Units : Minimum Order Quantity 5 and Multiples thereof
Units : Minimum Order Quantity 5 and Multiples thereof