
Interchangeable oral-nasal Endotracheal Tube
This novel innovation is the world’s first oral/ nasal interchangeable endotracheal tube. It offers a method to change between an oral endotracheal tube to a nasal endotracheal tube (and vice versa) without reintubation, while ventilation is maintained.
This method is ideal for use in maxillofacial surgery, where both oral and nasal intubation may be required. It is suitable for initial intubation of trauma patients in the emergency department over a bougie or with a stylet, where nasal intubation may be later required for maxillofacial surgery or patient transport. It provides a secure endotracheal tube/ airway for ventilation of children in ICU. It is also useful in managing a difficulty airway when intubating over a bougie or fibre optic scope.

Benefits of the interchangeable oral-nasal endotracheal tube include:
After initial orotracheal intubation continued intubation and ventilation allows for all subsequent steps to be performed in a safe, controlled manner.
Interchangeable oral/nasal endotracheal tube negates the need for extubation and reintubation.
The risk of bleeding and secretions from manipulation of an endotracheal tube through the nasopharynx making intubation difficult is removed.
Atraumatic nasal intubation with soft, flexible and blunt introducer attached to flexible reinforced airway tubing has been shown to reduce the risks associated with nasal intubation.
Flexible reinforced airway tubing allows intubation through the safer lower nasal pathway.
A safe method of nasotracheal intubation for those practitioners not skilled in the art of standard nasotracheal intubation.
No need for airway exchange catheters.
All Genesis airway endotracheal tubes have posterior facing bevels shown to be safer when passed through the nasopharynx and to provide a greater initial success rate of intubation when railroaded over a bougie or fibreoptic scope.
All Genesis airway endotracheal tubes have high volume low pressure cuffs to seal the airway without trauma.The reinforced endotracheal tubes are manufactured with soft, smooth PVC with a non stick finish allowing easy railroading over a bougie or scope.
All Genesis airway endotracheal tubes have a curved atraumatic bevelled tip preventing hang up on laryngeal structures when used with a bougie or fibre optic scope.
Studies that support the use of the interchangeable oral-nasal endotracheal tube include:
Contraindications to Nasal-endotracheal Intubation
Suspected base of skull fractures
Bleeding diathesis
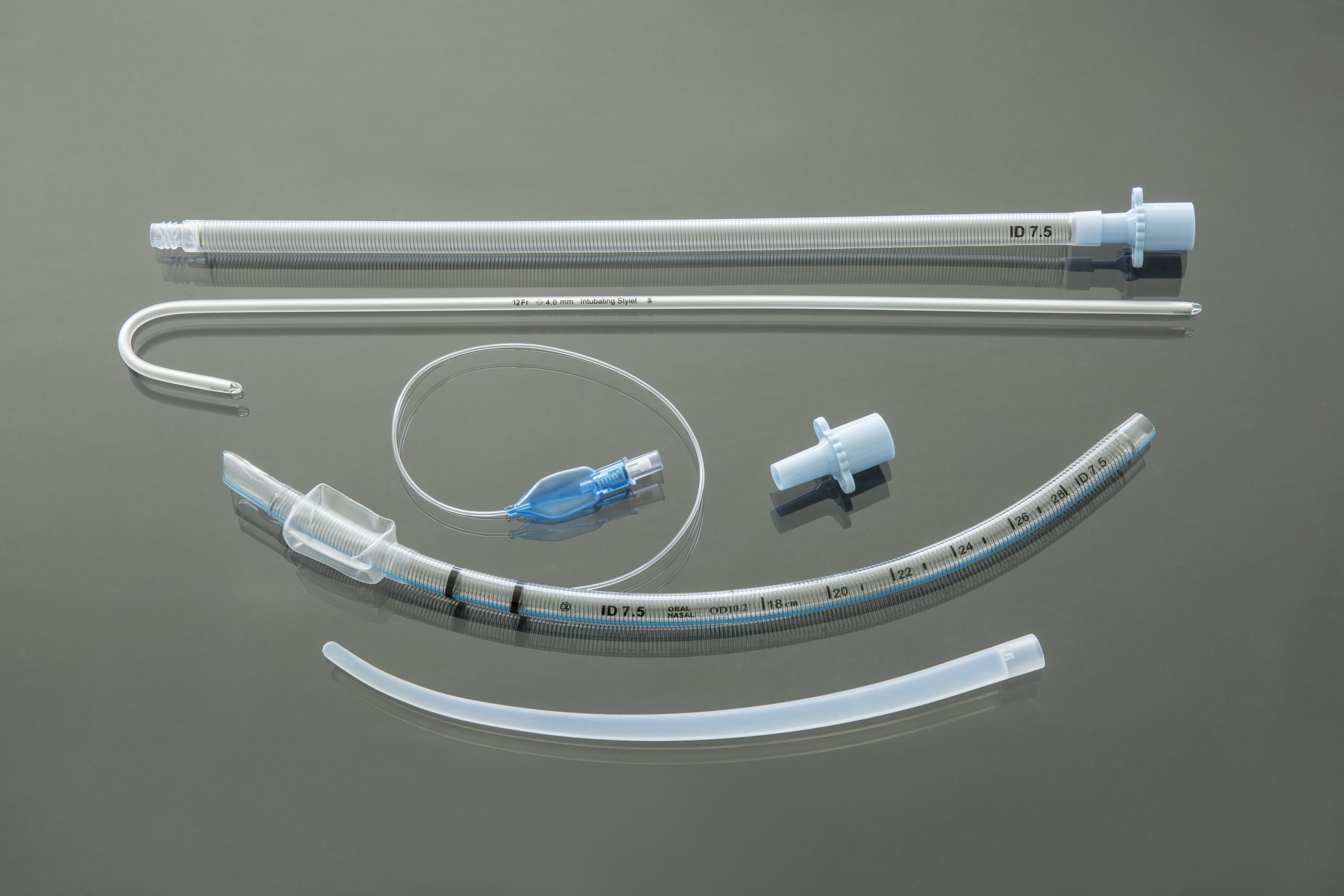
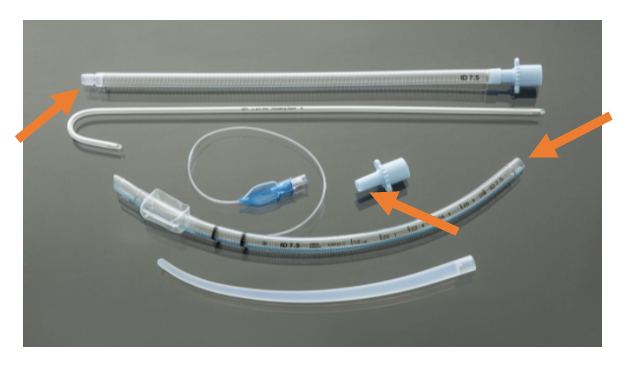
Our interchangeable oral-nasal endotracheal tube is presented as a pack containing:
Flexible reinforced endotracheal tube with a posterior facing bevel, modified cuff inflation line insertion and a removable 15 mm ISO connector.
Flexible reinforced airway tubing having a fixed 15 mm ISO connector and a connector to mate to an Introducer.
Malleable stylet.
Introducer.
Insertion of the interchangeable oral/nasal ETT requires an assistant and an anaesthesiologist.
NO Lubrication is to be applied to the 15mm connectors or the connections of the introducer, airway tubing or laryngeal mask airway tubing or possible disconnection can occur in the procedure.
ORAL to NASAL ETT
The reinforced ETT is used to secure the airway through the mouth. Anaesthesia is maintained and the patient ventilated.
A Bite block is inserted between the molar teeth to keep the mouth open.
The distal end of the flexible reinforced airway tubing is connected with the introducer*.
The introducer is passed through the most patent nostril. Using a laryngoscope, the introducer is visualized in the oropharynx. It is then grasped and delivered through the mouth by simultaneously pulling the end of the introducer with Magill’s forceps, while the assistant pushes the airway tube through the nose. Once approximately 5cm of the airway tubing protrudes from the lips, the introducer is removed.
The anaesthetic circuit is then removed from the oral ETT and connected to the proximal end of the nasal airway tubing. The 15mm connecter is removed from the oral ETT tubing and the tubing is joined to the distal end of the airway tubing* protruding through the mouth. Both ventilation and anaesthesia are maintained.
The Anaesthesiologist then stabilizes the ETT by grasping the ETT in the oropharynx with Magill’s forceps.
The redundant loop of airway tubing of the joined ETT and nasal airway tubing is reduced by gentle traction on the nasal airway tubing distal to the nose by the assistant while the anaesthesiologist simultaneously guides the loop pushing it through the mouth while stabilizing the ETT with the other hand.
Once satisfied that the ETT remains in the correct position and ventilation is maintained the nasal airway tubing is disconnected from the ETT and the 15mm connector is reinserted in the ETT and reconnected to the airway circuit. The pilot balloon and tubing may be stored in the mouth if necessary.
NASAL TO ORAL LARYNGEAL ETT
The anaesthetic circuit is removed from the nasal ETT along the 15mm connector The ETT is stabilized int the larynx by grasping the ETT in the oropharynx with Magill’s forceps. The ETT distal to the nose is pushed back through the nostril until the end is at the nares, creating a loop in the oropharynx. Using the index finger of the other hand the anaesthesiologist hooks it behind the ETT in the oro-pharynx . By pulling it out the mouth, it is delivered through the nasal passage. The 15mm connector is reinserted and anaesthetic circuit is connected to the ETT allowing continued ventilation and anaesthesia.
It is recommended that the bite block remains in use until the Nasal ETT is now reconfigured as the original oral ETT.
FOR EMEGENCY REMOVAL OF NASAL ETT
Cut and remove the ETT pilot balloon and inflation valve that remains in the oral cavity and then remove the nasal ETT by pulling out through the nose.
IT IS ADVISED THAT YOU WATCH THE VIDEOS DEMONSTRATING THE USE OF DONETT:
Units : Minimum Order Quantity 5 and Multiples thereof