
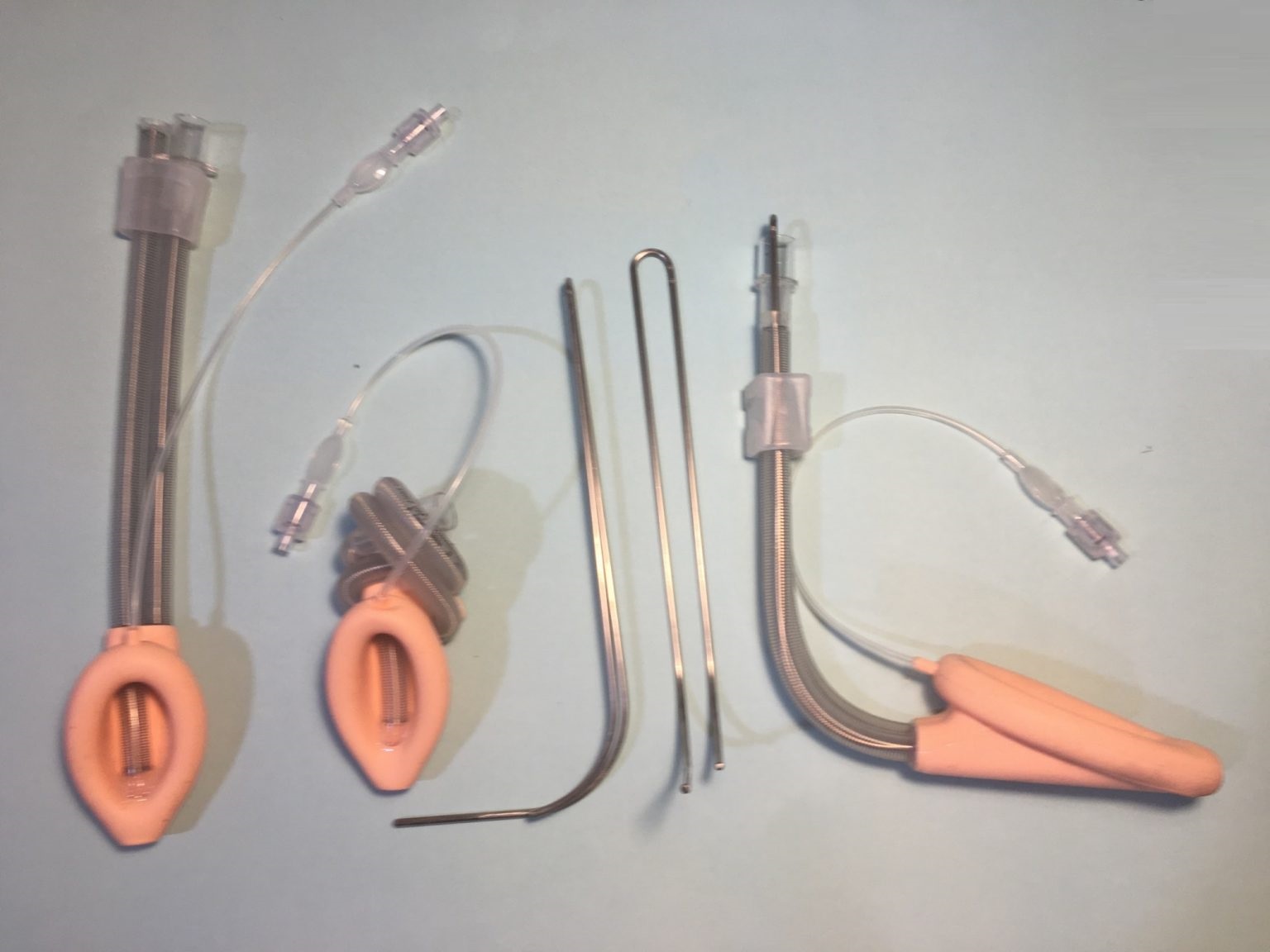
Flexi – 2G SAD with Sliding Bite Block
The first single-use, second generation, flexible laryngeal mask airway.
Flexi – 2G SAD with Sliding Bite Block is differentiated from other second generation SAD’s by having a flexible wire‐reinforced airway tube and separate flexible wire‐reinforced drainage tube that allows it to be positioned away from the surgical field. It may be particularly useful in procedures where the surgeon and anaesthesiologist are working in the same area, such as procedures involving the mouth, head or neck.
The flexibility of the airway tube provides an easy connection at any angle from the mouth. The tube may be relocated from side-to-side during the surgical procedure, without loss of seal of the cuff against the larynx.
The sliding bite block allows the airway tube to be easily repositioned for surgical access and prevents airway occlusion and negative pressure pulmonary oedema caused by the patient biting down on the airway tube.
Has a wide bore gastric drainage channel made of reinforced tubing (preventing collapse of the tube particularly when suction is applied) allowing easy insertion of a nasogastric tube and facilitates drainage of large volumes of gastric regurgitated fluids.



Flexi-2G SAD is versatile – one supraglottic airway device that ticks all the boxes:
Flexible laryngeal mask airway
2nd generation laryngeal mask airway - single use
Improved pharyngeal seal - improved ventilation pressures
Improved gastric seal – reduced risk of aspiration
Large volume #7 reinforced gastric drain tube
Easy insertion and reduced risk of mal-positioning #7 reinforce drainage tube extends to oesophageal port
Easy insertion of large bore nasogastric tube – drain tube ID 7mm
Able to intubate through the laryngeal mask airway with the use of an Aintree Intubating catheter
Conforms to difficult airways where anatomically shaped rigid tubes fail
Suitable for paediatric use
Suitable for use in prone position
Potential Problems with a 1ST GENERATION FLEXIBLE SAD
difficult to insert-hard to manipulate into larynx with single flexible tube
leakage with positive pressure ventilation
risk of gastric insufflation and aspiration
Advantages of a 2ND GENERATION FLEXIBLE SAD
Data show that specific features of the 2nd Generation laryngeal mask airway may reduce the risk of pulmonary aspiration compared with the 1st Generation laryngeal mask airway
This is primarily due to the addition of
– Improved pharyngeal seal enabling controlled ventilation at higher airway pressures
– Increased oesophageal seal, which lessens the likelihood of regurgitant fluids entering the pharynx and leading to aspiration
– A drain tube which lies over the top of the oesophagus when the laryngeal mask airway is correctly positioned. This may be used to:
- Assist insertion
- Confirm correct device positioning
- Enable access to the stomach
- Alert the user to the presence of regurgitation
- Enable gastric contents to safely bypass the oropharynx and exit the patient
- Easier insertion having 2 reinforced tubes attached to the mask gives more stability and manoeuvrability and prevents the mask of the supra glottic airway device folding over resulting in mal-positioning on insertion.
What is NAP4?
NAP4 is the largest study of major complications of airway management ever performed.
A year-long national service evaluation, endorsed by all four Chief Medical Officers of the UK, collected data between September 2008 and August 2009.
The NAP4 report demonstrates that:
Among airway management devices (ETT – FM – laryngeal mask airway) laryngeal mask airways were associated with a lower reported incidence of major airway complications per million than other devices
Cases of death/brain damage reported to NAP4 were ETT 9.1/million; FM 6.5/million; SAD 5.0/million
The majority of laryngeal mask airway-related complications were aspiration
In all but one case (second generation device, non-inflatable cuff), aspiration via an laryngeal mask airway occurred with a first-generation device
The NAP4 report1 made three key recommendations on the use of second generation laryngeal mask airways:
NAP4 Recommendations:
If tracheal intubation is not considered to be indicated but there is some (small) increased concern about regurgitation risk, a SECOND GENERATION SUPRAGLOTTIC AIRWAY is a more logical choice than a first generation one.
In patients considered to be at low risk of aspiration who have other factors that mean that use of an laryngeal mask airway is at the limits of normality (e.g. patient position, access to the airway, patient size) consideration should be given to use of a SECOND GENERATION LARYNGEAL MASK AIRWAY.
In view of the above recommendations, and the frequency of these circumstances, it is recommended that all hospitals have SECOND GENERATION LARYNGEAL MASK AIRWAYS available for both routine use and rescue airway management.
Introducer for the Flexi-2G SAD
The introducer transforms the flexible laryngeal mask airway into an anatomically curved laryngeal mask airway for introduction and placement in the larynx.
Features:
The introducer is totally contained within the reinforced tubing of the airway and gastric tube preventing any mucosal contact or injury.
The dual prongs of the introducer prevent rotation of the laryngeal mask in the pharynx.
The reinforce airway tubing and introducer in the airway tubing prevents the mask folding over while being placed.
Sizes:
Indicated by bars etched on metal arm
How to use the Introducer with the Flexi-2G SAD

Increased risk of aspiration: Prolonged bag-valve-mask ventilation, morbid obesity, second or third trimester pregnancy, patients who have not fasted before ventilation, upper gastrointestinal bleed
Need for high airway pressures; poor pulmonary compliance, high airway resistance
Suspected or known abnormalities in supraglottic anatomy
The cuff inflation must be checked before use.
Place on a flat surface then deflate the mask cuff with a syringe.
Lubricate the back plate of the mask.
Make sure the patients head is in the “sniffing the morning air” position.
Insert the laryngeal mask along the hard and soft palate, guiding the mask through the natural bend in the airway until resistance is felt.
Create a seal by inflating the mask cuff and check the pressure.
Check the mask inflation pressure every 30 minutes, particularly if nitrous oxide is used.
Confirm the mask is placed correctly and the patient ventilation is adequate. (The suprasternal notch tap test or the “Brimacombe bounce” confirms the location of the tip in the oesophagus behind the cricoid cartilage.)
Units : Minimum Order Quantity 10 and Multiples thereof