
Nasal Laryngeal Mask Airway
This novel innovation is the world’s first commercial nasal laryngeal mask. It allows good surgical access for dental, maxillofacial, ear nose and throat, head and neck surgery.
Laryngeal masks are easier to insert compared to endotracheal tubes.
Airway is first secured with an oral flexible reinforced laryngeal mask airway before nasal intubation.
Airway and ventilation is maintained throughout procedure.
Complications are minimised as:
The airway is first secured orally before nasal intubation.
The introducer and flexible reinforced airway tubing used for nasal intubation are recognised to reduce complications of nasal intubation.
The flexible reinforced endotracheal tube allows nasal intubation through the lower safer nasal passage.
Airway is more secure using a nasal laryngeal mask airway compared to the use of an oral laryngeal mask airway for oral surgical procedures.
Well tolerated and may be removed in recovery room improving operating room efficiency
Use of a laryngeal mask airway compared to Endotracheal intubation results in reduced:
post operative nausea and vomiting
post operative sore throat
coughing on emergence
haemodynamic instability
anaesthetic requirements
recovery time for day surgery

Use only if suitably experienced in the use of laryngeal mask airways in airway management.
CONTRAINDICATIONS TO NASAL-ENDOTRACHEAL INTUBATION:
Suspected base of skull fractures.
Bleeding diathesis.
CONTRAINDICATIONS TO USING A FIRST GENERATION LARYNGEAL MASK AIRWAY:
Increased risk of aspiration: Prolonged bag-valve-mask ventilation, morbid obesity, second or third trimester pregnancy, patients who have not fasted before ventilation, upper gastrointestinal bleed.
Need for high airway pressures; poor pulmonary compliance, high airway resistance.
Suspected or known abnormalities in supraglottic anatomy.
CONTRAINDICATIONS FOR USING NASAL LARYNGEAL MASK AIRWAY:
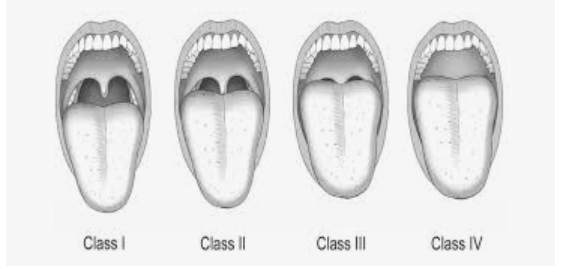
Only use in patients with Mallampati oropharyngeal views of grade 1 and 2 to allow direct vision of introducer and laryngeal mask airway tubing in oropharynx.
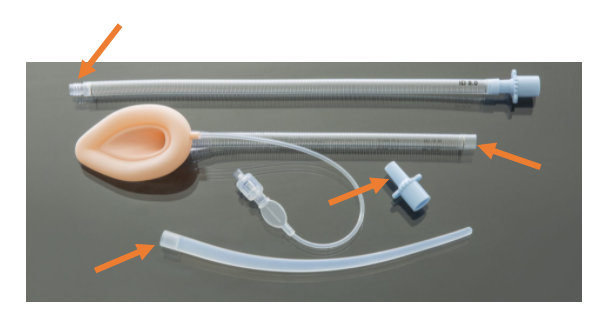
OUR NASAL LARYNGEAL MASK AIRWAY IS PRESENTED AS A PACK CONTAINING:
Flexible reinforced laryngeal mask airway with a removable 15 mm ISO connector.
Flexible reinforced airway tubing having a fixed 15 mm ISO connector and a connector to mate to an Introducer.
Introducer.

THE CORRECT USE OF THE NASAL LARYNGEAL MASK AIRWAY REQUIRES AN ASSISTANT AND AN ANAESTHESIOLOGIST.
NO lubrication is to be applied to the 15mm connectors or the connectors of the introducer, airway tube or laryngeal mask airway tube or disconnection may occur during the procedure.
The flexible reinforced laryngeal mask airway is used to secure the airway through the mouth. Anaesthesia is maintained and the patient ventilated.
A Bite block is inserted between the molar teeth to keep the mouth open.
The distal end of the flexible reinforced airway tubing is connected with the introducer.
The introducer is passed through the most patent nostril. Using a laryngoscope the introducer is visualized in the oropharynx, it is then grasped and delivered through the mouth by simultaneously pulling the end of the introducer with Magill’s forceps while the assistant pushes the airway tube through the nose. Once approximately 5cm of the airway tubing protrudes from the lips the introducer is removed.
The anaesthetic circuit is now removed from the oral laryngeal mask airway and connected to the proximal end of the nasal airway tubing. The 15mm connecter is removed from the oral laryngeal mask airway tubing and the tubing is joined to the distal end of the airway tubing protruding through the mouth. Ventilation and anaesthesia are maintained.
The Anaesthesiologist then stabilizes the mask of the laryngeal mask airway in the larynx by grasping the airway tubing in the oropharynx with Magill’s forceps or by using the middle and index fingers of the non-dominant hand on the junction of the mask and airway tubing.
The redundant loop of airway tubing of the joined laryngeal mask airway and nasal airway tubing is reduced by gentle traction on the nasal airway tubing distal to the nose by the assistant while the anaesthesiologist simultaneously guides the loop, pushing it through the mouth while stabilizing the mask in the larynx with the other hand.
Once satisfied that the laryngeal mask is in the correct position and ventilation is maintained the nasal airway tubing is disconnected from the laryngeal mask tubing and the 15mm connector is reinserted in the laryngeal mask airway tubing and reconnected to the airway circuit. The pilot balloon and tubing may be stored in the mouth if necessary.
NASAL TO ORAL LARYNGEAL MASK (Reversal)
The anaesthetic circuit is removed from the nasal laryngeal mask along the 15mm connector. The mask is stabilized in the larynx by grasping the airway tubing in the oropharynx with Magill’s forceps, or by using the middle and index fingers of the non-dominant hand on the junction of the mask and airway tubing. The laryngeal mask airway tubing distal to the nose is pushed back through the nostril until the end is at the nares creating a loop in the oropharynx. Using the index finger of the other hand the anaesthesiologist hooks it behind the airway tubing loop of the laryngeal mask airway in the oro-pharynx. By pulling it out the mouth it is delivered through the nasal passage. The 15mm connector is reinserted and the anaesthetic circuit is connected. An oral laryngeal mask airway has been reconfigured. It is recommended that the bite block remains in use until the Nasal laryngeal mask airway is now reconfigured as the original oral laryngeal mask airway.
FOR EMEGENCY REMOVAL OF NASAL LARYNGEAL MASK AIRWAY
Remove the 15mm connector. Grasp the airway tubing of the Nasal laryngeal mask airway in the oro-pharynx through the mouth with Magill’s forces or by hooking a finger behind the tubing and pulling it through the mouth delivering both the laryngeal mask airway mask from the larynx and the tubing from the nose.
IT IS ADVISED THAT YOU WATCH THE VIDEOS DEMONSTRATING THE USE OF THE NASAL LARYNGEAL MASK AIRWAY

SIZES BASED ON STANDARD SAD CUFF SIZES:
Units : Minimum Order Quantity 5 and Multiples thereof